The POWERSPINE Team

Dr. Florian Maria Alfen
International Spinal Specialist

Sebastian Färber
Board of the International Society for Medical Strengthening Therapy
Graduate sports scientist

Anton Högele
Graduate sports scientist
Business economist

Bruno Domokos
Doctoral Researcher in Sport Science and Lecturer at the University of Würzburg

ANATOMY
We are aware today, that chronic back pain usually is the result of a weak autochthonous back musculature. These muscles play a key role in stabilizing the spine and upright posture, but can not be tensed deliberately. They are inherent and generally don´t need exercise. However the increasing sedentary lifestyle, the lack of exercise in every day life or a pain-related relieving posture cause the weakening of the autochthonous musculature an as a result of the entire spine. In contrast to superficial muscles, which can be trained in a fitness center, the autochthonous spine muscles can only be exercised through isolated muscle training. The Powespine training machines enable us to build up cervical as well as lumbar spine musculature without any interference of surrounding muscles. Meaning that the superficial musculature is excluded through specific fixation and ergonomic features of the machines. So the cause of back pain can be eliminated.
")

SCIENCE

Source: Bachelor thesis in collaboration with the Julius-Maximilians-University Würzburg – Institute of Sports Sciences
Authors: Dr. Christoph Spang, Elena Sophia Barth, Daniela Pia Köber, Witold Golonka, Sandra Ort
Overview of the latest scientific literature:
Atrophy and fatty infiltration of the paraspinal back muscles are major causes for chronic back and neck pain
Multiple studies have shown that paraspinal back muscles play a key role in stabilizing the spine (Steele et al., 2014). A weakening (atrophy) of these muscles is considered to be a risk factor for developing acute and chronic back pain (Steele et al., 2015a). In contrast, a specific and isolated training of this muscle group can minimize this risk and avoid pain (Steele et al., 2015a). Morphological studies have revealed a much higher degree of atrophy and fatty infiltration in patients with chronic back and neck pain compared to healthy individuals (Fernandez-de-las-Penas et al., 2008; Eliott et al., 2014; Teichthal et al., 2015a). Furthermore, the corticomotor control is impaired in most patients (Masse-Alerie et al., 2016). These morphological and neuromuscular changes potentially cause an increasing lack of stability in the spine eventually leading to the development of disk herniations and degenerative disorders (stenosis, spondyl arthritis etc.) (Ekin et al., 2016; Fortin et al., 2017; Hicks et al., 2009). It can thus be concluded that healthy paraspinal muscles are essential for maintaining back health.
.
Sports activities in general only have limited effect on chronic pain conditions
Several studies have demonstrated that lack of physical activity leads to an increasing instability in the spine and increases risks for future back pain (Teichthal et al., 2015b). This correlation seems to even be higher with increasing with age (Dahlqvist et al., 2017; Hicks et al., 2009). Despite this clear connection, it has been shown that physical activity as therapeutic measure only has limited efficiency. Studies on high-level athletes have revealed multiple cases with paraspinal atrophies and chronic back pain. It seems that high frequencies of physical activity and the presence of well-developed skeletal muscles do not prevent from developing chronic back pain (Hides et al., 2008; Wassermann et al., 2018). It can thus be concluded that for successful rehabilitation treatment options need to focus on targeting the deep paraspinal back muscles.
Isolated training of paraspinal back muscles using a fixation system
The results of multiple studies have shown that exercise programs that strengthens the paraspinal muscles are capable to relief the pain symptoms (Hides et al., 2008; Steele et al., 2015b). Due to its primary function for upright positioning and stabilizer for the spine, paraspinal back muscles cannot be contracted voluntarily. Therefore, isolated training performed with high intensities is very challenging. Other muscle groups such as the hip extensors commonly carry big parts of the load so that training stimulus for the paraspinal muscles is significantly minimized (Steele et al., 2015b). During the last two decades intensive research has been performed in order to develop training machines that decrease the activity of other muscle groups. Optimal results were achieved using a fixation system that is the basis of the Dr. Alfen therapy devices. Via a dorsal pelvic stabilization and through semi-sitting positioning the hip extensors and lower limb muscles are deactivated (da Silva et al., 2009; San Juan et al., 2005; Larivière et al., 2010). The same principles were applied in the development of the training devices for the neck region (Schomacher & Falla, 2013; Pollock et al., 1993). It seems that maximal training stimulus leading to local muscles exhaustion can only be achieved using this fixation system. Information on current strength levels and potential deficits can be gained from isometric strength tests (Graves et al., 1990a,b; Robinson et al., 1992)
For optimal results and low-risk training protocols need to be adapted to the patients’ diagnoses
Due to acute pain it is often not possible to exercise with high intensities und within a large range of motion (ROM). Therefore we strongly recommend adapting the ROM and the training weights to the current symptoms and the underlying morphological changes in the spine. Interestingly, this does not lead to a reduced efficiency. Studies have shown that training within a limited ROM does eventually have therapeutic effects on the full ROM (Graves et al., 1992; Steele et al., 2013). Therefore, training protocols can be adapted to the underlying diagnoses. From our experience the right choice and optimal progression of ROM and weights are essential for optimal rehabilitation. We have developed a system (Alflexus Software) that contains pre-settings for more than 240 spinal diagnoses. Using this system, a therapist can optimally guide training progression and at the same time guarantee low risk for the patient. That is especially crucial when the patient has advances structural changes in the spine (disk herniation, stenosis, spondyle arthristis etc.).
Training frequency and intensity
According to the literature available, 1-2 high intensity training sessions a week and maximum muscle fatique are sufficient to achieving ideal therapy results (Steele et al., 2015a,b; Graves et al., 1990b; Pollock et al., 1989). Intriguingly enough, the number of sets is irrelevant, so one high intensity set each training session is sufficient to reaching maximum exhaustion. However the current pain condition and wellbeing has to be considered when increasing the weight. Also the therapy has to be started with submaximum intensity. To achieve lasting results, the patient has to complete all 18 training sessions. However as previously described, the adjustment of the patient to structural modifications is a crucial factor in achieving a successfull rehabilitation. Patients that suffer from a disc prolapse for example, have to be trained differently than patients suffering from degenerative spine diseases.
Clinical outcome
Scientifically it is evident that isolated extension resistance training provides superior results for rehabilitating patients from back pain than any other type of exercise (Steele et al., 2015a). It appears to be sufficient and effective for significant and meaningful improvements in perceived pain and disability (Steele et al., 2017; Pollock et al., 1993; Evans et al., 2002). This clinical outcome is associated with increased isometric lumbar extension strength (Steele et al., 2018). These findings are supported by a recent study by Steele and co-workers in which it has been shown that intervertebral discs can heal and regenerate with medical strengthening therapy (Steele et al., 2015c).
Research findings of the Dr. Alfen Team
In an unpublished study from our clinic, 88% of patients reported improvements in pain symptoms (Spang et al., 2017; Alfen & Spang, 2017). These results are astonishing as the patient material included many patients with severe and advanced spine disorders.
Summary:
Therapy concept as well as training machines are based on latest scientific findings and are ideal tools to efficiently treat acute and chronic neck and back pain. Through continuous exchange with scientists and cooperating universities the quality of our therapy is monitored and if needed improved.
PARTNER
LITERATURE
Dr. Alfen Team
- SpangC, Wagenblast, Haas D, Alfen F. Clinical outcome of isolated lumbar extension resistance training for chronic lower back pain – a retrospective study on 626 patients; presented on Eurospine Congress, 2017, Dublin, Ireland.
- AlfenF, Spang C. Isolated extension exercise and Transforaminal Endoscopic Surgery (TES) as treatment concept for chronic back pain; presented on BIT’s 4thAnnual World Congress of Orthopaedics, 2017, Taiyuan, China
Other Sources
- Da SilvaRA, Larivière C, Arsenault AB, Nadeau S, Plamondon A. Pelvic stabilization and semisitting position increase the specificity of back exercises. Medicine and Science in Sports and Exercise. 2009; 41(2):435-43.
- DahlqvistJR, Vissing CR, Hedermann G, Thomsen C, Vissing J. Fat Replacement of Paraspinal Muscles with Aging in Healthy Adults. Medicine and Science in Sports and Exercise. 2017; 49(3):595-601.
- EkinEE, Kurtul Yildiz H, Mutlu H. Age and sex-based distribution of lumbar multifidus muscle atrophy and coexistence of disc hernia: an MRI study of 2028 patients. Diagnostic and Interventional Radiology. 2016; 22(3):273-6.
- ElliottJM, Pedler AR, Jull GA, Van Wyk L, Galloway GG, O’Leary SP. Differential changes in muscle composition exist in traumatic and nontraumatic neck pain. Spine. 2014; 39(1):39-47.
- EvansR, Bronfort G, Nelson B, Goldsmith CH. Two-year follow-up of a randomized clinical trial of spinal manipulation and two types of exercise for patients with chronic neck pain. Spine. 2002; 27(21):2383-9.
- Fernandez-de-las-PenasC, Albert-Sanchis JC, Buil M, Benitez JC, Alburquerque-Sendin F. Cross-sectional area of cervical multifidus muscle in females with chronic bilateral neck pain compared to controls. The Journal of Orthopaedic and Sports Physical Therapy. 2008; 38(4):175-80.
- FortinM, Lazary A, Varga PP, Battie MC. Association between paraspinal muscle morphology, clinical symptoms and functional status in patients with lumbar spinal stenosis. European Spine Journal. 2017; 26(10):2543-51.
- GravesJE, Pollock ML, Carpenter DM, Leggett SH, Jones A, MacMillan M, et al. Quantitative assessment of full range-of-motion isometric lumbar extension strength. Spine. 1990a ;15(4):289-94.
- GravesJE, Pollock ML, Foster D, Leggett SH, Carpenter DM, Vuoso R, et al. Effect of training frequency and specificity on isometric lumbar extension strength. Spine. 1990b ;15(6):504-9.
- GravesJE, Pollock ML, Leggett SH, Carpenter DM, Fix CK, Fulton MN. Limited range-of-motion lumbar extension strength training. Medicine and science in sports and exercise. 1992;24(1):128-33.
- HicksGE, Morone N, Weiner DK. Degenerative lumbar disc and facet disease in older adults: prevalence and clinical correlates. Spine. 2009 ;34(12):1301-6.
- HidesJA, Stanton WR, McMahon S, Sims K, Richardson CA. Effect of stabilization training on multifidus muscle cross-sectional area among young elite cricketers with low back pain. The Journal of Orthopaedic and Sports Physical Therapy. 2008 ;38(3):101-8.
- LarivièreC, DA Silva RA, Arsenault AB, Nadeau S, Plamondon A, Vadeboncoeur R. Specificity of a back muscle exercise machine in healthy and low back pain subjects. Medicine and Science in Sports and Exercise. 2010; 42(3):592-9.
- Le CaraEC, Marcus RL, Dempsey AR, Hoffman MD, Hebert JJ. Morphology versus function: the relationship between lumbar multifidus intramuscular adipose tissue and muscle function among patients with low back pain. Archives of Physical Medicine and Rehabilitation. 2014;95(10):1846-52.
- Masse-AlarieH, Beaulieu LD, Preuss R, Schneider C. Corticomotor control of lumbar multifidus muscles is impaired in chronic low back pain: concurrent evidence from ultrasound imaging and double-pulse transcranial magnetic stimulation. Experimental Brain Research. 2016; 234(4):1033-45.
- PollockML, Graves JE, Bamman MM, Leggett SH, Carpenter DM, Carr C, et al. Frequency and volume of resistance training: effect on cervical extension strength. Archives of Physical Medicine and Rehabilitation. 1993; 74(10):1080-6.
- PollockML, Leggett SH, Graves JE, Jones A, Fulton M, Cirulli J. Effect of resistance training on lumbar extension strength. American Journal of Sports Medicine. 1989; 17(5):624-9.
- RobinsonME, Greene AF, O’Connor P, Graves JE, MacMillan M. Reliability of lumbar isometric torque in patients with chronic low back pain. Physical Therapy. 1992; 72(3):186-90.
- San JuanJG, Yaggie JA, Levy SS, Mooney V, Udermann BE, Mayer JM. Effects of pelvic stabilization on lumbar muscle activity during dynamic exercise. Journal of Strength and Conditioning Research. 2005; 19(4):903-7.
- SchomacherJ, Falla D. Function and structure of the deep cervical extensor muscles in patients with neck pain. Manual Therapy. 2013; 18(5):360-6.
- SteeleJ, Bruce-Low S, Smith D, Jessop D, Osborne N. A randomized controlled trial of limited range of motion lumbar extension exercise in chronic low back pain. Spine. 2013;38(15):1245-52.
- SteeleJ, Bruce-Low S, Smith D. A reappraisal of the deconditioning hypothesis in low back pain: review of evidence from a triumvirate of research methods on specific lumbar extensor deconditioning. Current Medical Research and Opinion. 2014; 30(5):865-911.
- SteeleJ, Bruce-Low S, Smith D. A review of the clinical value of isolated lumbar extension resistance training for chronic low back pain. PM R. 2015a; 7(2):169-87.
- SteeleJ, Bruce-Low S, Smith D.A review of the specificity of exercises designed for conditioning the lumbar extensors. British Journal Sports Medicine. 2015b; 49(5):291-7.
- SteeleJ, Bruce-Low S, Smith D, Osborne N, Thorkeldsen A. Can specific loading through exercise impart healing or regeneration of the intervertebral disc? Spine J. 2015; 15(10):2117-21.
- SteeleJ, Bruce-Low S, Smith D, Jessop D, Osborne N. Isolated Lumbar Extension Resistance Training Improves Strength, Pain, and Disability, but Not Spinal Height or Shrinkage (“Creep”) in Participants with Chronic Low Back Pain. Cartilage. 2017c; 1:1947603517695614.
- SteeleJ, Fisher J, Perrin C, Conway R, Bruce-Low S, Smith D. Does change in isolated lumbar extensor muscle function correlate with good clinical outcome? A secondary analysis of data on change in isolated lumbar extension strength, pain, and disability in chronic low back pain. Disability and Rehabilitation.2018;12:1-9.
- TeichtahlAJ, Urquhart DM, Wang Y, Wluka AE, Wijethilake P, O’Sullivan R, Cicuttini FM. Fat infiltration of paraspinal muscles is associated with low back pain, disability, and structural abnormalities in community-based adults. Spine J. 2015a; 15(7):1593-601.
- TeichtahlAJ, Urquhart DM, Wang Y, Wluka AE, O’Sullivan R, Jones G, Cicuttini FM. Physical inactivity is associated with narrower lumbar intervertebral discs, high fat content of paraspinal muscles and low back pain and disability. Arthritis Research & Therapy. 2015b; 17:114.
- WassermanMS, Guermazi A, Jarraya M, et al. Evaluation of spine MRIs in athletes participating in the Rio de Janeiro 2016 Summer Olympic Games. BMJ Open Sport & Exercise Medicine. 2018; 4:e000335.
THE POWERSPINE CONCEPT

POWERSPINE BACK AND NECK
ALFLEXUS SOFTWARE:
Ganzheitliche Konzeptsoftware entwickelt auf der Basis von über 450.000 Trainings-Einheiten
POWERSPINE ACADEMY
QUALITY MANAGEMENT
SUPPORT:
Eröffnungsvortrag, Telefonsupport, Onlinepräsenz, Jährlicher Kundenkongress und vieles mehr zur ständigen Unterstützung des Kunden
LICENSES
POWERSPINE TRAINING DEVICES
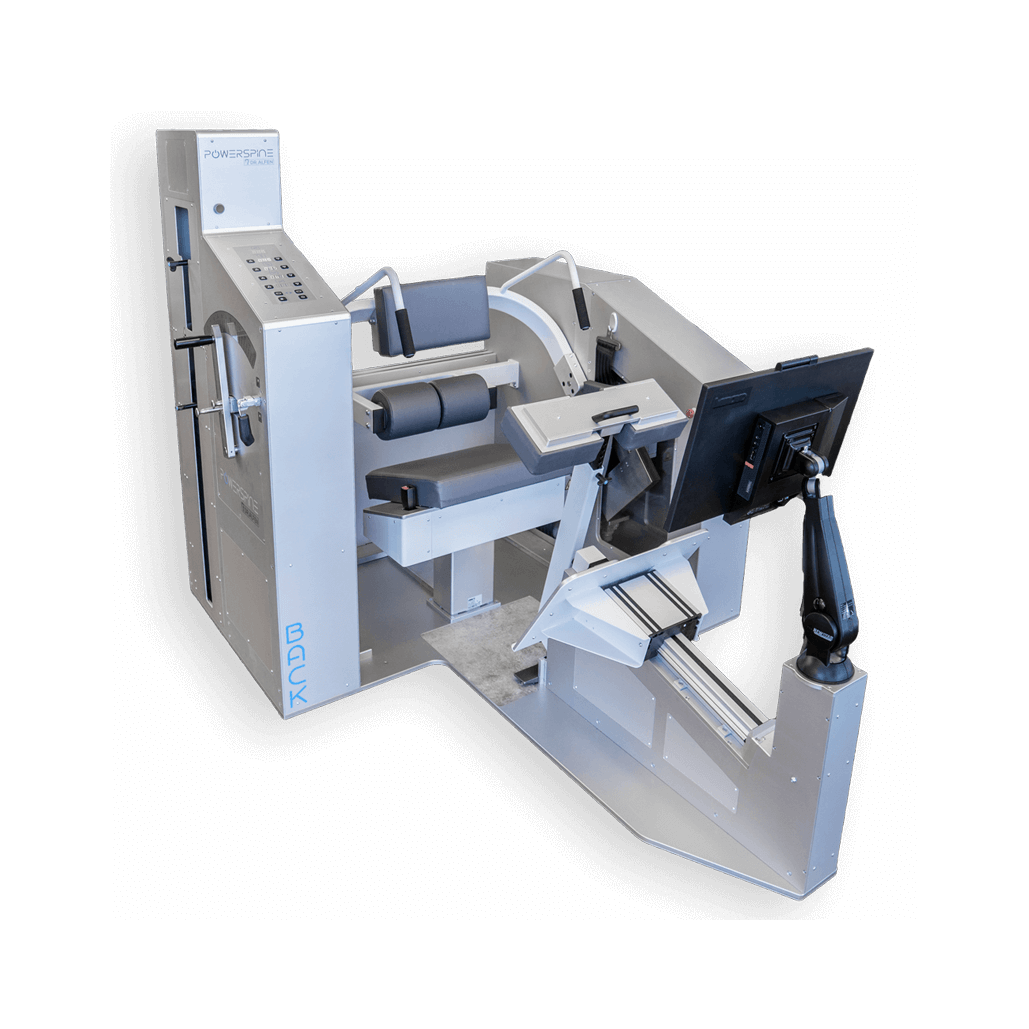
POWERSPINE back:
Training of the deep autochthonous lumbar spine
muscles:
The ergonomic sitting position an the numerous
possibilities to individually secure the lower
extremities, enable to train the lower autochthonous back muscles without the interference of surrounding synergists.
Size (LxWxH): 2225 x 1600 x 1600 mm
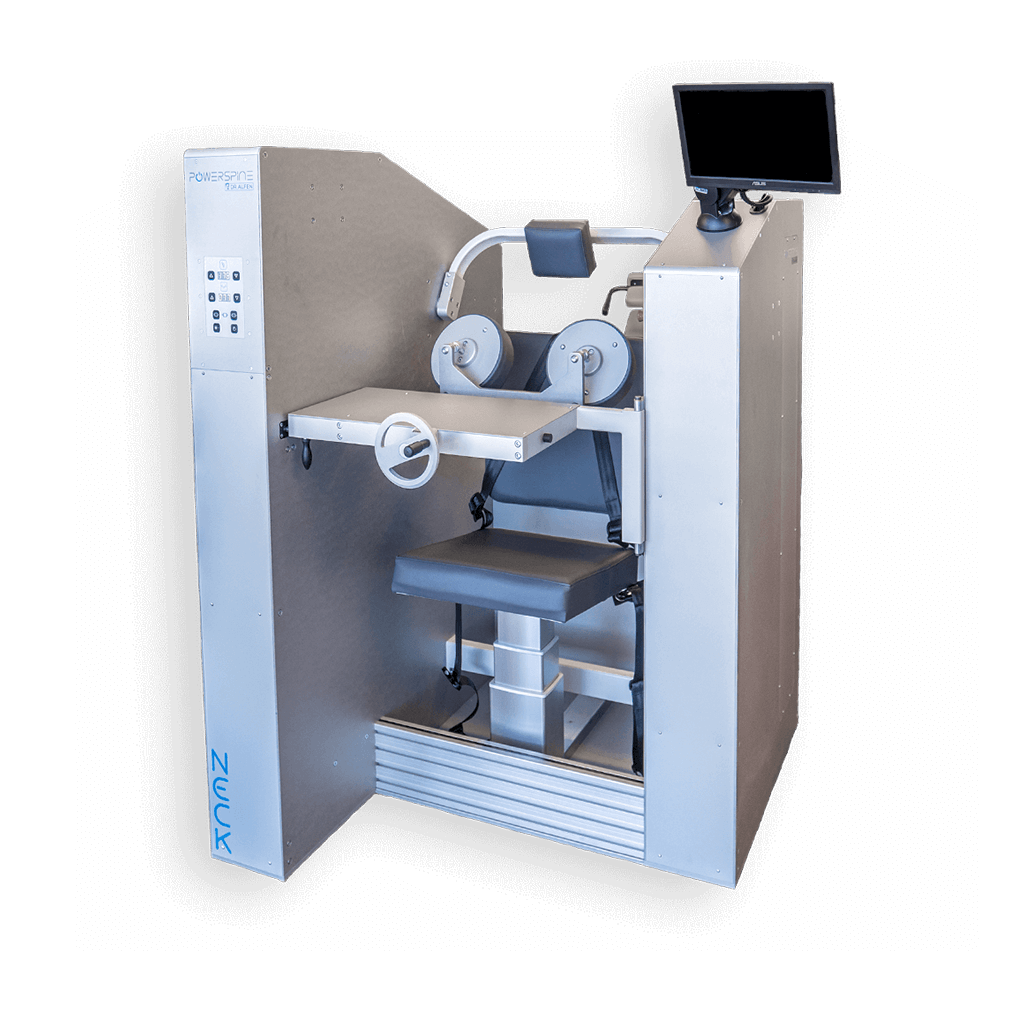
POWERSPINE neck:
The ergonomic sitting position and the numerous
possibilities to individually secure the upper body, enable to train the upper autochthonous back muscles without interference of surrounding synergists. .
Size (LxWxH): 1200 x 1500 x 1700 mm
FACTS:
✓ Electric height adjustment of footrest as well as head cushion and upper body cushion
✓ Electric adjustment of the pelvic strap
✓ Electric determination of the counter weight
✓ Accessible entry without barriers
✓ Particularly quiet electric engines
✓ Ideal ergonomic sitting position
✓ Higly efficient training without performance peaks
✓ Position of angulation by laser pointer
✓ Inbuilt touchscreens
✓ Swift installation through modular construction
POWERSPINE ACADEMY
POWERSPINE Concept operators usually receive an extensive instruction into the concept, preparing them for practical use in their establishment. Among others, this instruction includes anatomic and exercise physiological basics, as well as exercise training sessions. Finally the participants take a theoretical and practical examination to receive their training certificate. What occupational groups are able to perform the training, has to be discussed beforehand in a personal conversation.
FACTS:
✓ Intensive training for therapists in the Academy or inhouse
✓ Detailed theoretical and practical contents
✓ Theoretical and practical examination
✓ Certified training by the International Society for Medical Strengthening Therapy
✓ Multilingual training if required

QM – SUPPORT – LICENSES

Quality management and process optimisation are significant to the POWERSPINE Concept and are therefore ensured trough multiple visits at the clients location. Furthermore our telephone support is always available for any questions. With the exclusive customer portal there is the possibility of marketing documents, scientific studies and graphics, animation videos and much more to download. ✓ Regular quality management at each location
With the regular Alfexus software updates our customers always stay up to date and benefit from the latest optimizations.
Annual congresses where all POWERSPINE operators can exchange their experiences and get insight into new developments. Each operator obtains territorial protection for their area, as well as various marketing materials.
FACTS:
✓ Process optimisation by exchange of experience
✓ Annual international meeting for operators
✓ Alflexus software updates
✓ Telephone support
✓ Exclusive customer portal containing numerous templates and further information
PROCEDURE
OF THE POWERSPINE CONCEPT

Check-up
Starting the Powerspine
Concept with a personal conversation to a spinal specialist about your specific afflictions.

Personal Training
Every training session is guided by qualified personnel to ensure an effective and safe training.

Muscle function test
The muscle function test takes place at the beginning as well as during the last training session. Each strength level is compared to individuals without spinal disorders.

Training
Standard training sets include 18 sessions on the machines. Each session lasts 150 seconds, 2-3 times a week. To preserve the training results, only one session each month is required.
POWERSPINE
OVERVIEW

Back pain of all kinds
Disc prolapses and disc protrusions
Tension in cervical as well as lumbar spine
Chronic pain
Head aches, migraines and tinnitus
Muscular imbalances
Post surgery
Osteoporosis
Rheumatic diseases
Degenerative changes of the spine
Whiplash and fractures
Postural weaknesses and dysfunctions
HOW THE
POWERSPINE BACK UND NECK WORK

PROCEDURE
OF THE POWERSPINE CONCEPT
Check-up
Starting the Powerspine
Concept with a personal conversation to a spinal specialist about your specific afflictions.
Personal Training
Every training session is guided by qualified personnel to ensure an effective and safe training.
Muscle function test
The muscle function test takes place at the beginning as well as during the last training session. Each strength level is compared to individuals without spinal disorders.
Trainingsablauf
Standard training sets include 18 sessions on the machines. Each session lasts 150 seconds, 2-3 times a week. To preserve the training results, only one session each month is required.
COOPERATION PARTNERS

International Society for Medical Strengthening Therapy

Northern Ontario School of Medicine

University Würzburg

University of cooperative education

CONTACT
APPLICATION FORM